Disruptions in Histaminergic Transmissions in Narcolepsy
This content was developed using literature published in peer-reviewed journals and other materials.
Disruptions in Histaminergic Transmissions in Narcolepsy
This content was developed using literature published in peer-reviewed journals and other materials.
Overview
A postmortem study showed increases in histaminergic-producing neurons in those with significant loss of orexin (hypocretin).1
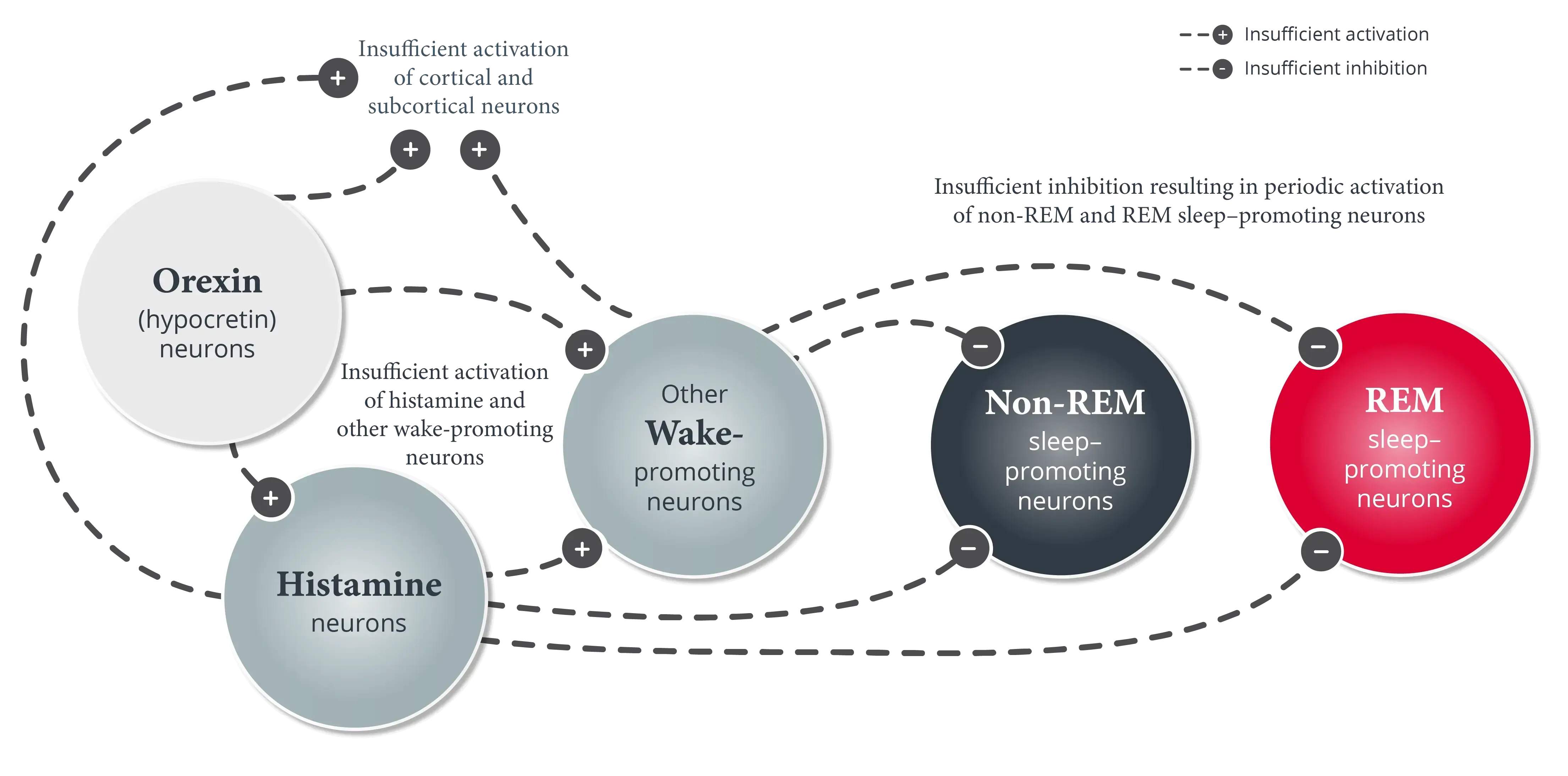
It is widely documented that patients with narcolepsy—approximately 95% with narcolepsy type 1 (narcolepsy with cataplexy) and approximately 10% with narcolepsy 2 (narcolepsy without cataplexy)—are deficient in orexin (hypocretin).2-3
However, the potential involvement of another key wake-promoting neurotransmitter in the pathophysiology of narcolepsy is often overlooked.1
A postmortem study showed selective increases of histaminergic neurons in patients with narcolepsy type 1, characterized by loss of orexin (hypocretin) neurons, whereas the numbers of others, such as melanin-concentrating hormone (MCH)-producing neurons, remain unaffected.1
In the same study, patients with narcolepsy type 1 had almost twice as many histaminergic neurons as those without narcolepsy.1,*
- Within this group, a subset of patients with the largest amount of orexin (hypocretin) loss (>90%) had the highest measurement of histaminergic neurons compared to the patients with less severe orexin (hypocretin) cell loss1


Imaging studies also observed that patients with narcolepsy type 1 had increased volume in parts of the hypothalamus, including the TMN—the only neuronal source of histamine in the brain compared to controls.5-7,† One possible explanation for this larger size is the increased number of histaminergic neurons housed there.5
Despite observed increases in the numbers of histaminergic neurons seen in the postmortem study, other studies have documented significant reductions in histamine levels found in the cerebrospinal fluid (CSF) of patients with narcolepsy compared with control subjects. These reductions are8,9:
- Present in patients with narcolepsy regardless of hypocretin deficiency status and the presence of cataplexy‡
- More pronounced in patients with narcolepsy and low CSF hypocretin-1 compared to those with normal CSF hypocretin-1§
In pediatric patients with narcolepsy type 1, higher levels of histamine in the CSF, lower levels of CSF t-MeHA, and lower t-MeHA/HA ratios have been observed.10
Additional research is needed to better characterize the changes in histamine in patients with loss of orexin (hypocretin).
*Based on a postmortem study of 19 subjects (7 patients with narcolepsy with cataplexy and 12 controls). The number of hypothalamic neurons producing orexin (hypocretin), MCH, and histamine (histaminergic neurons were identified using immunostaining for histidine decarboxylase) were counted using immunohistochemical and stereological techniques.1
†Based on an imaging study comparing MRI-based volumes of the whole hypothalamus and 10 hypothalamic subregions in patients with narcolepsy type 1 and controls (N=54 patients with post H1N1 narcolepsy type 1 and 114 controls).5
‡Cross-sectional study comparing CSF histamine levels in patients with narcolepsy (n=67), idiopathic hypersomnia (n=26), obstructive sleep apnea (n=16), and neurological controls (n=73).8
§Study comparing the CSF levels of histamine in patients with narcolepsy with low CSF hypocretin-1 (n=34) and normal CSF hypocretin-1 (n=24), selected from the Stanford Narcolepsy Database, and normal controls (n=23).9
HA, histamine; MRI, magnetic resonance imaging; t-MeHA, tele-methylhistamine.
References
- Valko PO, Gavrilov YV, Yamamoto M, et al. Increase of histaminergic tuberomammillary neurons in narcolepsy. Ann Neurol. 2013;74(6):794-804.
- American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd ed, text revision. American Academy of Sleep Medicine; 2023.
- Mahoney CE, Cogswell A, Koralnik IJ, Scammell TE. The neurobiological basis of narcolepsy. Nat Rev Neurosci. 2019;20(2):83-93.
- John J, Thannickal TC, McGregor R, et al. Greatly increased numbers of histamine cells in human narcolepsy with cataplexy. Ann Neurol. 2013;74(6):786-793.
- Juvodden HT, Alnæs D, Lund MJ, et al. Larger hypothalamic volume in narcolepsy type 1. Sleep. 2023;46(11):zsad173. doi:10.1093/sleep/zsad173
- Haas HL, Sergeeva OA, Selbach O. Histamine in the nervous system. Physiol Rev. 2008;88(3):1183-1241.
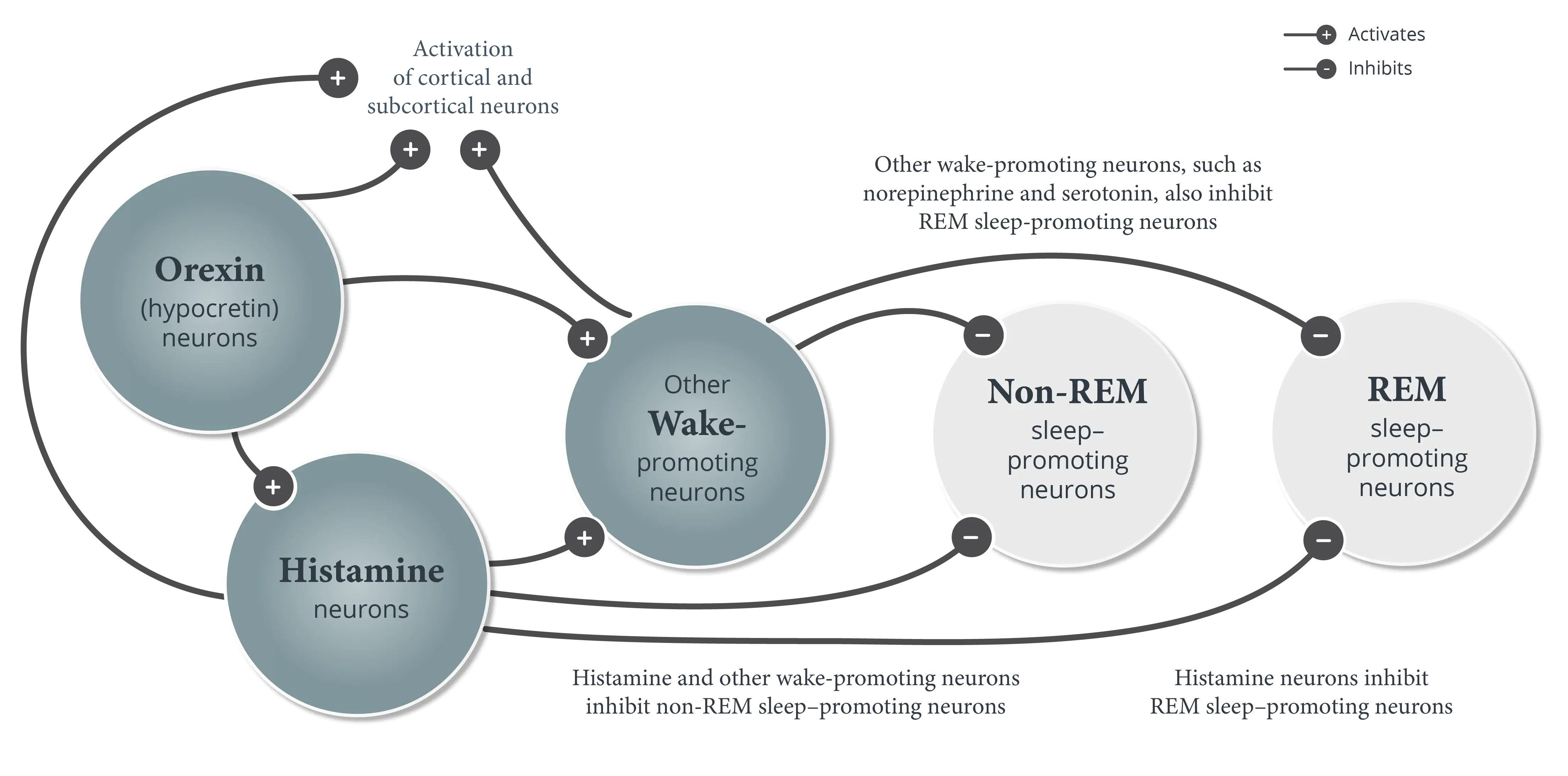
- Scammell TE, Arrigoni E, Lipton JO. Neural circuitry of wakefulness and sleep. Neuron. 2017;93(4):747-765.
- Kanbayashi T, Kodama T, Kondo H, et al. CSF histamine contents in narcolepsy, idiopathic hypersomnia and obstructive sleep apnea syndrome. Sleep. 2009;32(2):181-187.
- Nishino S, Sakurai E, Nevsimalova S, et al. Decreased CSF histamine in narcolepsy with and without low CSF hypocretin-1 in comparison to healthy controls. Sleep. 2009;32(2):175-180.
- Franco P, Dauvilliers Y, Inocente CO, et al. Impaired histaminergic neurotransmission in children with narcolepsy type 1. CNS Neurosci Ther. 2019;25(3):386-395.